



Overview of Grant Award and Application Requirements
The Juvenile Accountability Block Grants (JABG) Program, administered at the federal level by the Office of Juvenile Justice and Delinquency Prevention (OJJDP), supports state and local efforts to reduce juvenile crime through programs that focus on offender accountability (Public Law 107-273). As the designated state agency for this federally funded program, the Corrections Standards Authority (CSA) will distribute the 2009 annual allocations to those local jurisdictions meeting the federal funding threshold to receive a direct allocation. The grant year will cover July 1, 2009 through June 30, 2010.
Due Date: This application is due to the CSA via e-mail by May 28, 2009.
What’s New This Year: California’s State Advisory Committee on Juvenile Justice and Delinquency Prevention (SACJJDP), which oversees the use of federal funds administered by CSA, identified five priority areas in their Strategic Plan on which California will focus its efforts for the next three years. The five priority areas are Alternatives to Detention, Disproportionate Minority Contact, Evidence-Based Practices, Restorative Justice, and Holistic Approaches to Offender Counsel.
JABG discretionary funds have been identified by the SACJJDP and the CSA to support the priority area of Evidence-Based Practices. Toward that end, CSA has developed a”Best Practices Approach Initiative” to support programs rated Exemplary, Effective and Promising as defined in the OJJDP Model Programs Guide. The goal of this initiative is to assist probation departments and other JABG eligible recipients in developing and increasing their knowledge and use of best practices in the field of juvenile justice.
Using evidence-based practices (i.e., research-based and proven programs to deal with the issues of juvenile offending and correction) within the context of best practices involves the following:
1. Organizational development to create a culture that is accepting of best practices and evidence-based approaches.
2. The development of collaborations, oriented to best practices and evidence-based approaches within the juvenile justice system.
3. The use of validated risk/needs assessment tools to determine corrections and rehabilitation case planning.
4. The use of evidenced-based practices and programs to produce positive criminal justice and juvenile rehabilitative and developmental outcomes.
5. Data collection and analysis to monitor program processes and outcomes.
6. Performance management for ongoing assessment and improvement of programs and practices.
7. Quality assurance assessments to ensure fidelity to proven models and adherence to standards of care.
8. A focus on sustainability to ensure continuation of successful programs and practices after the termination of outside funding.
CSA is issuing this Request for Proposals (RFP) to identify an expert trainer to develop and deliver numerous services related to evidence-based, best, and promising practices. The services include conducting statewide regional trainings, a comprehensive review of projects, providing organizational development and supporting system change to agencies seeking enhanced resources. The training assistance will be offered to JABG eligible recipients and probation departments throughout the state.
JABG recipients will have the opportunity to participate in the statewide training and comprehensive review of current validated assessment tools and best practices that will be conducted in the coming year. Participation in these efforts will not affect your direct allocation this year; however, the SACJJDP plans to encourage JABG recipients to align the use of their direct allocation with goals that are identified in the SACJJDP’s Strategic Plan for the future.
Eligible Applicants: Units of local government meeting the minimum federal funding threshold are eligible to apply for the formula-based direct allocation. Please refer to Appendix A for a listing of eligible units of local government, including the federally determined grant amount for each. Localities shall designate an implementing agency for the grant project.
Local Match: Applicants must assure that they will contribute a cash match of 10% of the total project costs (see Appendix A for required match amounts based on the federal formula). Applicants opting to use JABG funds to construct new and permanent detention facilities must provide a 50% cash match. Matching funds may be either state or local dollars. Federal funds are not an allowable match source.
Eligible Expenditures: Grantees must expend JABG funds for projects that fall within the 17 federally designated program purpose areas, with a focus on juvenile accountability. Please see Appendix B for information on the JABG program purpose areas and performance measures.
Disbursement of Grant Funds: Disbursement of grant funds occurs on a reimbursement basis for actual project costs incurred during a reporting period. Grantees must submit invoices on line to the CSA on a quarterly basis, within 45 days following the end of the reporting period. Grantees must maintain adequate supporting documentation for all costs, both grant and match, claimed on invoices.
Federal Performance Measures: Federal regulations require JABG grantees to select a program purpose area(s) from the JABG program list and report specific data pertaining to the area(s) identified. Grantees will report data to the CSA on a quarterly basis via progress reports.
Local Advisory Board: Under federal law, a local advisory board must review a Coordinated Enforcement Plan (CEP) outlining how JABG funds will be expended. For the purpose of this grant, this application is the CEP. The board must include, if appropriate, representatives from the police, sheriff and probation departments, district attorney’s office, juvenile court, education, social services, a nonprofit and nongovernmental victim advocacy organization, and a nonprofit religious or community group. Grantees may use an existing advisory board with similar membership (e.g., Juvenile Justice Coordinating Council) to meet this requirement.
Resolution: Applicants must submit a resolution from their governing board (City Council or Board of Supervisors) addressing specific requirements. Please see Attachment C for a Sample Resolution. The resolution must be on file with the CSA prior to a finalized grant award agreement.
Waivers: A qualifying unit of local government may waive its right to a direct grant award and request that such unit’s funds be awarded to and expended for its benefit by a larger or contiguous unit of local government. Please see Attachment D for the pertinent waiver documentation.
Complete Application Submittal: A complete application includes the application document, Federal Performance Measures form(s) and governing body’s resolution. Additionally, waiver documents are required from any applicant receiving funds waived from another locality.
Progress Reports: Grantees must submit quarterly progress reports, including the mandatory federal data and project progress notes, utilizing the JABG Progress Report form provided on the CSA website www.cdcr.ca.gov/Divisions_Boards/CSA/.
Audit: Grantees must submit an audit of expenditures within 120 days of the end of the grant period. Reasonable and necessary extensions to the timeframe may be granted if requested. Grantees may choose to submit either a program specific audit or a federal single audit.
Key Dates:
May 28, 2009 |
Applications due to CSA |
July 1, 2009 |
Grant year begins |
November 15, 2009 |
First quarterly progress report due covering July – Sept. 2009 First quarterly financial invoice due covering July – Sept. 2009 |
February 15, 2010 |
Second quarterly progress report due covering Oct. – Dec. 2009 Second quarterly financial invoice due covering Oct. – Dec. 2009 |
May 15, 2010 |
Third quarterly progress report due covering Jan. – Mar. 2010 Third quarterly financial invoice due covering Jan. – Mar. 2010 |
August 15, 2010 |
Fourth quarterly progress report due covering Apr. – June 2010 Fourth quarterly financial invoice due covering Apr. – June 2010 |
October 31, 2010 |
Final audit report due (unless extension granted) |
Contact and Program Information: Questions regarding this application process may be directed to Connie Lucero, Corrections Consultant for CSA, (916) 341-7392 or connie.lucero@cdcr.ca.gov. Further information about the JABG Program, including fiscal and progress reporting forms and the Grant Contract Administration and Audit Guide, is also available on the CSA’s web site at www.cdcr.ca.gov/Divisions_Boards/CSA/CPP/Grants/JABG/Index.html.

SECTION II: PROJECT INFORMATION |
A. PROJECT DESCRIPTION:
Part I: In the space below #5, provide the following project information:
1. Describe the project(s)/program(s) to be supported with JABG funds.
2. Define project goals and major activities/services.
3. Define the juvenile justice population(s) to be served by the project, including the estimated number of youth.
4. Support the project need with local data/information.
5. Describe staffing, including classification and number of staff required to achieve project goals.
1. The project supported by the JABG funds is the Victim Impact Awareness (VIA) Program. The purpose of this program is to educate youth who have victimized others about the impact that their actions have on others. This class, usually taught in 75-minute sessions over a seven-week period, is facilitated by staff from the Probation Department and from a non-profit counseling agency. Speakers are brought in to talk about their experiences as victims and videos are used to help youth to understand how their behavior impacts others.
2. Youth are required to complete a Behavior Contract in the first or second session, which includes what they will do to keep from victimizing others. They must attend at least five of the seven sessions but cannot miss the first and second. They are given a pre-test at the beginning and a post-test at the end to assess their change in understanding the impact their behavior had on the victim and the community. They are also referred to the Juvenile Mediation Program with the hope that they will mediate with their victim.
3. The population served will be any youth with a sustained law violation where there was a victim. The goal is to offer the class to 100 youth and to have 80 of those youth complete the program successfully.
4. A legal office specialist will keep track of attendance, completion of program requirements and number who complete the classes successfully. She will also check probation records to determine if those who completed the VIA Program re-offended during the grant period.
5. There will be at least four Probation staff and two therapists to support the two groups offered each quarter. There is also a Probation Supervisor that supports the program and a Legal Office Specialist responsible for enrollment, attendance and data collection. A Director is responsible for monitoring contracts, gathering all data and completing the quarterly progress reports. Our Financial Services Manager is responsible for processing invoices and completing quarterly financial progress reports.
Part II: Further identify the target population for your program by completing the table below. Place an “X” next to at least one population segment (or “not applicable”) in each of the six designated areas. Multiple boxes may be checked in any one area. Each “X” shall indicate the populations, if any, to which the program intends to offer targeted services. Targeted services include any services or approaches specifically designed to meet the needs of the population (e.g. gender specific, culturally based, developmentally appropriate services).
TARGET POPULATION | |
1. RACE |
4. AGE |
☐ Not applicable | |
X American Indian/Alaskan Native |
☐ Under 11 |
X Asian |
X 12-13 |
X Black/African American |
X 14-15 |
X Hispanic or Latino (of any race) |
X X16-17 |
X Native Hawaiian/Other Pacific Islander |
☐ 18 and over* |
X Other Race |
|
X White/Caucasian |
|
2. JUSTICE |
5. GEOGRAPHIC |
☐ At-Risk Population (no prior offense) |
☐ Not applicable |
X First Time Offenders |
☐ Rural |
X Repeat Offenders |
X Suburban |
☐ Sex Offenders |
☐ Tribal |
☐ Status Offenders |
☐ Urban |
X Violent Offenders |
|
3. GENDER |
6. OTHER POPULATIONS |
☐ Not applicable |
X Not applicable |
X Male |
☐ Mental Health |
X Female |
☐ Pregnant |
☐ Substance Abuse | |
☐ Truant/Dropout | |
*Participants 18 years and over must be under the jurisdiction of the juvenile justice system.
B. PROGRAM PURPOSE AREA(S): All funded projects must fall within one or more federally recognized purpose areas established for JABG. Appendix B includes a detailed listing of the 17 program purpose areas from which each applicant must choose. Each separate purpose area identified in this section will require subsequent data reporting on quarterly progress reports to the CSA. Applicants are encouraged to consolidate this portion as much as possible. In the space below, please indicate the selected program purpose area(s) by number and topic, and the federal dollar amount allotted to each. (Example: #8 Juvenile Drug Courts - $ 47,189)
#11 Accountability - $42,272
C. FEDERAL PERFORMANCE MEASURES: Grantees receiving over $10,000 must report data to the CSA on mandatory performance measures developed by the Office of Juvenile Justice and Delinquency Prevention. Once a purpose area(s) has been selected in Section II-B above, click below on the corresponding selection(s) and follow the directions for choosing the data to be reported. Data choices will appear in either one or both of these categories – direct service programs or system change programs. Grantees must first determine which category(s) best describes their project, as this will determine the data to be collected. Please note the Reporting Format column that prescribes the precise data to be collected.
Juvenile Accountability Block Grant (JABG)
Federal Juvenile Accountability Block Grant Logic Model PDF
Performance Measures:
Program Area 1: Graduated Sanctions PDF
Program Area 2: Corrections/Detention Facilities PDF
Program Area 3: Court Staffing and Pretrial Services PDF
Program Area 4: Prosecutors (Staffing) PDF
Program Area 5: Prosecutors (Funding) PDF
Program Area 6: Training for Law Enforcement and Court Personnel PDF
Program Area 7: Juvenile Gun Courts PDF
Program Area 8: Juvenile Drug Courts PDF
Program Area 9: Juvenile Records System PDF
Program Area 10: Information Sharing PDF
Program Area 11: Accountability PDF
Program Area 12: Risk and Needs Assessment PDF
Program Area 13: School Safety PDF
Program Area 14: Restorative Justice PDF
Program Area 15: Juvenile Courts and Probation PDF
Program Area 16: Detention/Corrections Personnel PDF
Program Area 17: Reentry PDF
![]()
SECTION III: BUDGET INFORMATION |
A. WAIVER AND MATCH CALCULATION: Completion of this segment of the budget section is only for those applicants receiving waivers of funding from other jurisdictions. Applicants not receiving waivers may skip to the next segment – part B of this budget section.
NOTE: The above Waiver and Match table is an Excel document. Double click on the document; fill in the numbers for auto calculation, then save.
B. BUDGET LINE ITEM TOTALS: Please complete the applicable fields in the following table for the proposed budget. Administrative overhead may not exceed 5% of the total grant funds requested. With the exception of new and permanent construction projects requiring a 50% cash match, the required cash match for all other projects is 10% of the total project costs. See Appendix A for pre-calculated 10% match amounts based on federal formula.
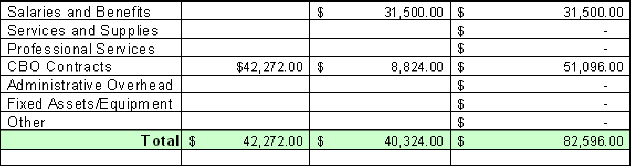
NOTE: The budget table is an Excel document. Double click on the document; fill in the numbers for auto calculation, then save.
C. BUDGET LINE ITEM DETAILS: Provide sufficient detail/breakdown to explain how the requested funds outlined in the table above will be expended in each applicable line item. Identify match items, their respective dollar amounts, and source of the match funds.
1. SALARIES AND BENEFITS: Number of staff, classification, salary and benefits.
Two (2) Deputy Probation Officers (DPO) co-facilitate classes with staff from our community based organizations. These DPOs also solicit speakers for the classes and provide support and follow-up to other DPOs.
2. SERVICES AND SUPPLIES: Includes leases, rent, utilities, travel and training.
0
3. PROFESSIONAL SERVICES: Includes evaluator, consultant services, therapists, and other professionals as required.
0
4. COMMUNITY-BASED ORGANIZATIONS: Name of organization and services to be provided.
Staff from North Peninsula Family Alternative and Youth and Family Enrichment Services will co-facilitate classes with Probation staff. Each agency will receive $25,548 for this program for fiscal year 2009-10.
5. ADMINISTRATIVE OVERHEAD: Indicate percentage and how calculated. This total may not exceed 5% of the grant funds.
0
6. FIXED ASSETS/EQUIPMENT: Office equipment, vehicles, other equipment necessary to perform program activities.
0
7. OTHER: Any other items not covered above but necessary to meet program goals.
0
SECTION IV: LOCAL ADVISORY BOARD |
In meeting the federal requirement, indicate in the spaces below the membership of the locally designated advisory board charged with reviewing the plan for expending JABG funds.
Date of meeting to approve application:
Name |
Title |
Agency |
Mark Raffaelli |
Chief of Police |
South San Francisco Police Dept |
Hector Acosta |
Detective |
San Mateo Co Sheriff’s Office |
James Wade |
Deputy District Attorney |
District Attorney’s Office |
Karen Philip |
Associate Superintendent |
Office of Education |
Kimberly Wheeler |
Exec. Director, Metal Health |
YMCA of San Francisco |
Margaret Copenhagen |
Lawyer |
Law Offices of MA Copenhagen |
Michael Garb |
Chief Executive Officer |
Youth & Family Enrichment Serv. |
Christine McGlynn |
Director |
San Mateo County Probation |
David Cherniss |
Juvenile Mediation Program Mgr. |
Victim Offender Mediation Program |
SECTION V: BOARD OF SUPERVISORS’ RESOLUTION |
As part of the grant application process, applicants must submit a resolution from the City Council/Board of Supervisors addressing specified issues. Please see Attachment C for a Sample Resolution. The resolution need not be submitted at the same time as the application document; however, the original resolution or copy thereof must be provided to the CSA prior to a grant award agreement being signed. Resolutions may be directed by mail to the JABG Coordinator, Connie Lucero at Corrections Standards Authority, 600 Bercut Drive, Sacramento 95811.
SECTION VI: AUDIT IDENTIFICATION |
Grant recipients must submit an audit of expenditures within 120 days following the end of the grant period. Grantees may choose either a program specific audit or a single federal audit. Federal guidelines allow grant recipients receiving $500,000 or more in federal funds (from all sources including pass-through sub-awards) in a fiscal year to use their federal juvenile justice grant funds to pay for the cost of the audit. Grantees falling below the $500,000 threshold must use non-federal funds (i.e., match funds) to pay for audit costs. For purposes of this application, please check one of the boxes below to indicate the grantee’s choice for meeting the audit requirement.
☐ In conformance with Federal OMB Circular #A-133, and the California State Controller’s Accounting Standards and Procedures Chapter 23, Grant Accounting Index, the identified grant will be included in the City/County Single Federal Audit Report, which will be submitted to the CSA within the required timeframe of 120 days from the end of the 12-month grant period. NOTE: Should an extension be needed, please provide in advance of the deadline a written justification that indicates reasons for the extension and the timeframe needed.
☒ In conformance with Federal OMB Circular #A-133, and the California State Controller’s Accounting Standards and Procedures Chapter 23, Grant Accounting Index, the grantee will provide a Program Specific Final Audit Report to the CSA within the required timeframe of 120 days from the end of the 12-month grant period.
![]()
PLEASE E-MAIL YOUR COMPLETED APPLICATION
BY MAY 28, 2009
to
Connie.Lucero @cdcr.ca.gov
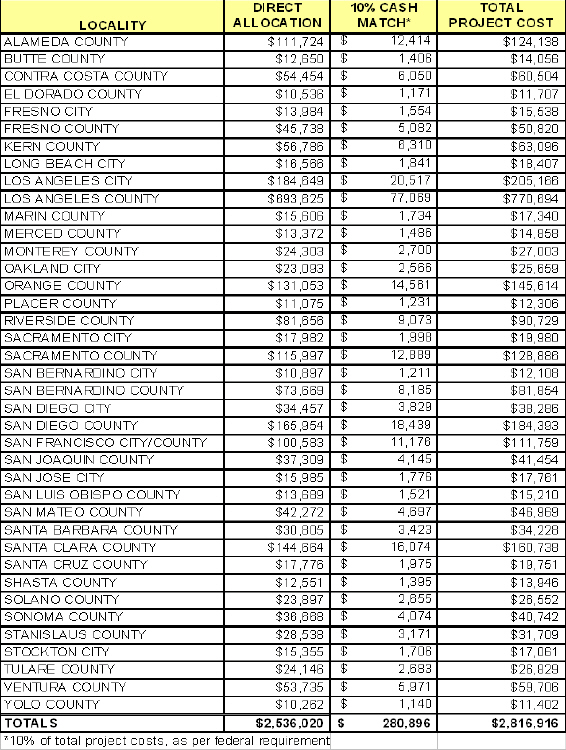
APPENDIX A – 09/10 DIRECT ALLOCATIONS FOR ELIGIBLE LOCALITIES
THE 09/10 DIRECT ALLOCATIONS ARE BASED ON CALIFORNIA’S 08/09 ALLOCATION
APPENDIX B – JABG PROGRAM PURPOSE AREAS
1) Graduated sanctions: Developing, implementing, and administering graduated sanctions for juvenile offenders.
2) Corrections/detention facilities: Building, expanding, renovating, or operating temporary or permanent juvenile corrections, detention or community corrections facilities.
3) Court staffing and pretrial services: Hiring juvenile court judges, probation officers, and court-appointed defenders and special advocates, and funding pretrial services (including mental health screening/assessment) for juvenile offenders to promote the effective, expeditious administration of the juvenile justice system.
4) Prosecutors (staffing): Hiring additional prosecutors so that more cases involving violent juvenile offenders can be prosecuted and backlogs reduced.
5) Prosecutors (funding): Providing funding to enable prosecutors to address drug, gang, and youth violence problems more effectively and for technology, equipment, and training to assist prosecutors in identifying and expediting the prosecution of violent juvenile offenders.
6) Training for law enforcement and court personnel: Establishing and maintaining training programs for law enforcement and other court personnel with respect to preventing and controlling juvenile crime
7) Juvenile gun courts: Establishing juvenile gun courts for the prosecution and adjudication of juvenile firearms offenders
8) Juvenile drug courts: Establishing drug court programs to provide continuing judicial supervision over juvenile offenders with substance abuse problems and to integrate administration of other sanctions and services for such offenders
9) Juvenile records system: Establishing and maintaining a system of juvenile records designed to promote public safety
10) Information sharing: Establishing and maintaining interagency information-sharing programs that enable the juvenile and criminal justice systems, schools, and social services agencies to make more informed decisions regarding the early identification, control, supervision, and treatment of juveniles who repeatedly commit serious delinquent or criminal acts.
11) Accountability: Establishing and maintaining accountability-based programs designed to reduce recidivism among juveniles who are referred by law enforcement personnel or agencies.
12) Risk and needs assessment: Establishing and maintaining programs to conduct risk and needs assessments of juvenile offenders that facilitate effective early intervention and the provision of comprehensive services, including mental health screening and treatment and substance abuse testing and treatment, to such offenders.
13) School safety: Establishing and maintaining accountability-based programs designed to enhance school safety.
14) Restorative justice: Establishing and maintaining restorative justice programs.
15) Juvenile courts and probation: Establishing and maintaining programs to enable juvenile courts and juvenile probation officers to be more effective and efficient in holding juvenile offenders accountable and reducing recidivism.
16) Detention/corrections personnel: Hiring detention and corrections personnel and establishing and maintaining training programs for such personnel, to improve facility practices and programming.
17) Reentry systems and programs: Establishing, improving and coordinating pre-release and post-release systems and programs to facilitate the successful reentry of juvenile offenders from state and local custody into the community.
ATTACHMENT C – SAMPLE RESOLUTION
Applicants must submit a resolution from the governing body (City Council/Board of Supervisors) that includes, at a minimum, the language and assurances outlined in the following sample:
WHEREAS the (insert name of applicant city/county) desires to receive and utilize federal grant funds available through the Juvenile Accountability Block Grants (JABG) Program administered by the Corrections Standards Authority (hereafter referred to as CSA).
NOW, THEREFORE, BE IT RESOLVED that the (insert title of designated official) is authorized on behalf of the (insert City Council/Board of Supervisors) to submit the JABG application and sign the Grant Agreement with the CSA, including any amendments thereof.
BE IT FURTHER RESOLVED that the (city/county) agrees to provide all matching funds required for said project, and abide by the statutes and regulations governing the JABG Program as well as the terms and conditions of the Grant Agreement as set forth by the CSA.
BE IT FURTHER RESOLVED that grant funds received hereunder shall not be used to supplant expenditures controlled by this body.
Passed, approved, and adopted by the (insert City Council/Board of Supervisors) of (insert name of city/county) in a meeting thereof held on (insert date) by the following:
Ayes:
Notes:
Absent:
Signature: Date:
Typed Name and Title:
ATTEST: Signature: Date:
Typed Name and Title:
ATTACHMENT D – WAIVER OF DIRECT GRANT AWARD
The following template/information must be provided on any waiver document submitted with a grant application. Original waiver documents must be submitted by mail to the Corrections Standards Authority (600 Bercut Drive, Sacramento, CA 95814).
I, (name/title), the legally authorized administrative officer (city manager or county administrator) representing the (name of waiving unit of local government) authorize the Corrections Standards Authority to transfer award funds allocated under the Juvenile Accountability Block Grants 2007 in the amount of $(grant amount) to (name of receiving unit of local government).
_____________________________________________
Authorized Official’s Signature
_________________________________________
Authorized Official’s Typed Name
_________________________________________
Authorized Official’s Typed Title
_________________________________________
Date Executed
Waiving unit of local government’s official seal or notary stamp is required below.