Education System Profile |
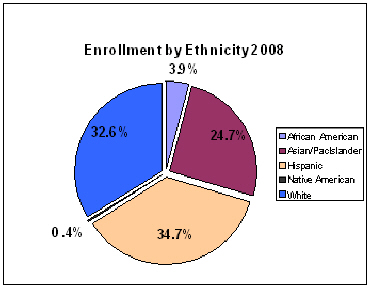
San Mateo County public school system is made up of 110 elementary, 31 middle and 30 high schools. Six continuation schools, mostly high school level, serve students with alternative approaches to better meet their needs. Total system enrollment is 88,974 students, and has experienced a 1% growth since 2006.6 Average class size is 24.8 which falls under the state average class size of 25.2. 7 The socio-economic make up of students mirrors the diversity of the general population. The trend in ethnic composition has changed over the last decade. The percentage of Caucasian students has declined, whereas Hispanic and Asian/Pacific Islander (PI) students make up larger proportions of the population. 8
Nearly one quarter of students are English language learners. The trend for the past 10 years demonstrates modest growth in comparison to the rate of enrollment. 97-98 02-03 07-08 10 -Year Trend Total Enrollment 92,763 88,991 88,974 -4.1% Spanish speaking 15.8% 17.9% 17.6% 1.8% Tagalog speaking 1.0% 0.9% 1.7% 0.7% All Other 4.7% 4.7% 4.4% -0.3% Total English Learners 21.5% 23.5% 23.7% 2.2% Although San Mateo County has a median income of $83,109 in 2008, the growth of poverty is evidenced by the increased participation in reduced price/free school lunch program. The rate of growth in the lunch programs surpasses the overall growth rate in California. In 2008, participation in San Mateo County was 32.9%. 9 |